(Good stuff, aside from being a rant against epidemiology which can only establish correlation, not causation)
Tactics without strategy is the noise before defeat. His holiness Sun Tzu
There is some risk involved in action, there always is. But there is far more risk in failure to act. His excellency Harry S. Truman
Now, imagine living your life without the ability to feed or bathe yourself, or walk a few blocks to meet friends for coffee. We take these for granted now, but to continue to live actively as we age, retaining even these minimal abilities, requires us to begin building a foundation of fitness and to maintain it diligently.

cms.gov (Medicare and Medicaid Services):
Activities of Daily Living (ADLs): Activities of daily living are activities related to personal care. They include bathing or showering, dressing, getting in and out of bed or a chair, walking, using the toilet, and eating. If a sample person has difficulty performing an activity by himself/herself and without special equipment, or does not perform the activity at all because of health problems, the person is deemed to have a limitation in that activity
| IADL | What it involves |
|---|
 |
| "We had come because rapamycin had been demonstrated to do something that no other drug had ever done before - extend maximum lifespan in a mammal. The discovery of rapamycin and the legacy of Dr. Surendra Nath (Suren) Sehgal |
I did the same by my meat, as well in regard to quantity as to quality, accustoming myself never to cloy my stomach with eating or drinking; but constantly rise from table with a disposition to eat and drink still more. In this I conformed to the proverb, which says, that a man, to consult his health, must check his appetite. (Discourses on the Sober and Temperate Life, Luigi Cornaro)
 |
| Luigi Cornaro, 15th century Italian architect, rich dude, afflicted with diseases of civilization, cured himself through calorie restriction. (autobiography) |
Aging is characterized by a progressive loss of physiological integrity, leading to impaired function and increased vulnerability to death,” wrote the authors of an influential 20l3 paper describing what they termed the “hallmarks of aging." Huey continued: “This deterioration is the primary risk factor for major human pathologies, including cancer, diabetes, cardiovascular disorders, and neurodegenerative diseases. His holiness Dr. Peter Attia
Stay active and watch the rate at which you put fructose into your system. Eating apples is okay, but drinking sport drinks will get you.
There is an incredible rush of anticipation one feels just before cutting through the last of several membranes separating the outside world from the inner abdominal cavity. One of the first things you see, as the incision grows, is the tip of the liver, which I've always considered to be a really underappreciated organ. Cool kids in medicine specialize in the brain or the heart. But the liver is the body's true workhorse and, also, it's simply breathtaking to behold. Normally, the healthy liver is a deep, dark, purply color, with a gorgeous silky-smooth texture.
More than one in four people on this planet have some degree of NASH (Non Alcoholic Steatohepatitis) or its precursor-NAFLD (Non Alcoholic Fatty Liver Disease). NAFLD is highly correlated with both obesity and Hyperlipidemia (excessive cholesterol) and often flies under the radar. Most patients are unaware that they have it and so are their doctors, because NAFLD and NASH have no obvious symptoms. The first signs would generally show up only on a blood test for the liver enzyme alanine amino-transferase (ALT for short)

As far back as the 1960's before obesity had become an epidemic, Stanford endocrinologist Dr. Gerald Reaven had observed that excess weight often travelled in company with certain other markers of poor health. He and his colleagues noted that heart attack patients often had both high fasting glucose levels and high triglycerides, as well as elevated blood pressure and abdominal obesity. The more of these boxes a patient checked, the greater their risk of cardiovascular disease. In the 1980s, Reaven labeled this collection of related disorders “Syndrome X"-where the X factor, he eventually determined, was insulin resistance. Today we call this cluster of problems “metabolic syndrome” (or MetSyn ), and it is defined in terms of five criteria:
- High BP (>130/85)
- High triglycerides (>150 mg/dl)
- Low HDL cholesterol (<40 mg/dl for men, 50 for women)
- Central adiposity (waist circumference > 40" in men or > 35" in women)
- Elevated fasting glucose (>110 mg/dl)
If you meet three or more, you have metabolic syndrome, along with 120m other Americans - according to 2020 article in JAMA.

Individual fat-storage capacity seems to be influenced by genetic factors. This is a generalization, but people of Asian descent, for example, tend to have a much lower capacity to store fat, on average, than Caucasians. There are other factors at play here as well, but this explains in part why some people can be obese but metabolically healthy, while others can appear “skinny” while still walking around with three or more markers of metabolic syndrome. It's these people who are most at risk, according to Mitch Lazar at U. Penn, because a"thin" person may simply have a much lower capacity to store fat.
Slightly fat person may have more metabolic leeway.
It doesn't take much visceral fat to cause problems. Let's say you are a forty-year-old man who weighs two hundred pounds. If you have 20 percent body fat, making you more or less average (50th percentile) for your age and sex, that means you are carrying 40 lbs of fat throughout your body. Now, even if just 4.5 lbs of that is visceral fat, you would be considered to be exceptionally high risk for CVD and type-2 diabetes-in the top 5% of risk for your age and sex.
 |
| How to get gout |
When we metabolize fructose in large quantities, a different enzyme takes over, and this enzyme does not put the brakes on ATP "spending" Instead, energy (ATP) levels inside the cell drop rapidly and dramatically. This rapid drop in energy levels makes the cell think "We are still hungry". Bottom line is that, even though it is rich in energy, fructose basically tricks our metabolism into thinking that we are depleting energy and need to take in still more food and store more energy as fat. This drop in cellular ATP triggers an enzyme called AMP-deaminase (the evil cousin of AMP-K (reverse fuel-gauge enzyme)). When AMP-K is activated, it triggers all sorts of cellular survival programs, including the burning of stored fat, that enable the organism to survive without food. When fructose triggers AMPD, on the other hand, it sends us down the path of fat storage. (This cascade also triggers hunger by blocking one Ieptin. )
On a more macro level, consuming large quantities of liquid fructose simply overwhelms the ability of the gut to metabolize it. The excess is shunted to the liver, where many of those calories are likely to end up as fat. Too many "healthy" fruit smoothies can do it (NAFLD).
For someone aged 36, my calcium CT score should have been 0. It was 6. Calcification of the arteries - atherosclerosis. Someone with a severe case could return a score well above 1000.

Anahad O'Connor calcium CT scan score 125 - very high! LPa-standard LDL particle fuses with another, rarer type of protein called apolipoprotein (a), or apo(a) for short ( not to be confused with apolipoprotein A or apoA, the protein that marks HDL.

Back when I had an office, I kept a clutter-free desk, but one book in particular was always there: Atlas of Atherosclerosis Progression and Regression, by Herbert C. Stary. It will never be a bestseller, but in the field of cardiovascular pathology it is legendary. It also happens to be a highly effective tool for communicating the seriousness of this disease to my patients, thanks to its lavish and gruesome photographs of arterial lesions as they form, develop and rupture-all taken from the arteries of dead people-many of them in their 20's and 30's.

Biggest Loser host Bob Harper's heart attack at age 52 was attributed to elevated levels of lipoprotein(a) (Lp(a)), according to a 2018 article in the Harvard Health Blog. Lp(a) is a fatty particle in the blood that carries cholesterol, fat, and proteins, and high levels can increase the risk of heart attacks and strokes. Harper's case highlighted the importance of testing for Lp(a), as it can be a significant risk factor even in physically fit individuals.
"I've been in the health and fitness industry for almost 30 years now, but I had to pivot my life and redefine the way that I ate and worked out." For starters, he now eats a largely Mediterranean diet. He says,"I went from eating a more high-protein, high-fat diet to being more balanced. I don't eat very much red meat anymore. I live on mostly fish, sometimes chicken, and lots of vegetables."
Not an atypical scenario: when a patient comes to me and says their father or grandfather or aunt, or all three, died of “premature" heart disease, elevated Lp(a) is the first thing I look for. It is the most prevalent hereditary risk factor for H disease, and danger amplified by fact that it's largely flying under the radar of medicine 2.0.
If you have a history of premature H attacks in your family, you should definitely ask for an Lp(a) test. We test all for Lp(a) during their first blood draw. Because elevated Lp(a) is largely genetic, it only need be done once. If everyone kept their LDL concentrations at their birth level, atherosclerosis might well be an orphan disease (something so rare that no one sees value in researching/developing-treatments-for it)

I knew that I wanted to be a surgical oncologist and that I had to work with Steve Rosenberg. Cancer had been on my mind since before I had even applied to medical school. During my post-bac year, while taking med school prerequisite courses, I volunteered on the pediatric cancer ward of Kingston General Hospital in Ontario, spending time with kids who were undergoing cancer treatment. Thankfully, childhood leukemia is one area where Medicine 2.0 has made real progress. But not all the kids survived, and the bravery of these children, the pain that they and their parents endured, and the compassion of their medical teams moved me more deeply than any engineering or mathematical problem. It confirmed my decision to switch from engineering to medicine.
Mustard gas used during WW1 was a direct precursor to some of the earliest chemotherapy agents, some of which are still in use. These drugs attack the replicative cycle of cells, and because cancer cells are rapidly dividing, the chemo agents harm them more severely than normal cells. But many important noncancerous cells are also dividing frequently, such as those in the lining of the mouth and gut, the hair follicles, and the nails, which is why typical chemotherapy agents cause side-effects like hair loss and gastrointestinal misery. Meanwhile, as cancer researcher Robert Gatenby points out, those cancer cells that do manage to survive chemotherapy often end up acquiring mutations that make them stronger, like cockroaches that develop resistance to insecticides.

The side effects of chemo might seem at the outset to be a fair trade for a "chance for a few more useful years". But.. The struggle is to convey the way that it hurt on the inside. I lay for days on end, trying in vain to postpone the moment when I would have to swallow. Every time I did swallow, a hellish tide of pain would flow up my throat, culminating in what felt like a mule kick in the small of my back.

For the last century or so, a handful of researchers have been investigating another unique property of cancer cells, and that is their metabolism. In the 19208, a German physiologist named Otto Warburg discovered that cancer cells had a strangely gluttonous appetite for glucose, devouring it at up to forty times the rate of healthy tissues. But these cancer cells weren't "respiring" the way normal cells do, consuming oxygen and producing lots of ATP, the energy currency of the cell, via the mitochondria. Rather, they appeared to be using a different pathway that cells normally use to produce energy under anaerobic conditions-meaning without sufficient oxygen, such as when we are sprinting. The strange thing was that these cancer cells were resorting to this inefficient metabolic pathway despite having plenty of oxygen available to them.
This struck Warburg as a very strange choice. In normal aerobic respiration, a cell can turn one molecule of glucose into as many as thirty-six units of ATP. But under anaerobic conditions, that same amount of glucose yields only two net units of ATP. This phenomenon was dubbed the Warburg effect, and even today, one way to locate potential tumors is by injecting the patient with radioactively labeled glucose and then doing a PET scan to see where most of the glucose is migrating. Areas with abnormally high glucose concentrations indicate the possible presence of a tumor.
Warburg was awarded the Nobel Prize in Physiology or Medicine in 1931 for his discovery of a crucial enzyme in the electron transport chain (a key mechanism for producing energy in the cell).
 |
| The Breakthrough: Immunotherapy and the Race to Cure Cancer by Charles Graeber |
James Allison of UT Houston figured out how cancer cells hide from the immune system by exploiting so-called checkpoints that are normally supposed to regulate our T-cells and keep them from going overboard and attacking our normal cells.
 |
| Specificity/sensitivity-the more you increase one, the more you decrease the other. |
The specificity of MRI is particularly reduced by glandular tissue. MRI is so good at detecting glandular cancer that it significantly overdoes it. The thyroid gland might be the worst offender of them all. I tell patients - if you're going to have a whole-body screening MRI, there is a good chance we'll be chasing down an insignificant thyroid or other nodule in exchange for getting such a good look at your other organs. As a result of this, about a quarter of my patients, understandably, elect not to undergo such screening.
Dr. Kellyann Niotis

This is why an important first step with any patient who may have cognitive issues is to subject them to a grueling battery of tests. One reason I like to have a preventive neurologist like Kellyann on staff, is that these tests are so complicated and difficult to administer, that I feel they are best left to specialists. They are also critically important to a correct diagnosis-assessing whether the patient is already on the road to AD or to another form of neurodegenerative dementia. These are clinically validated, highly complex tests that cover every domain of cognition and memory, including executive function, attention, processing speed, verbal fluency and memory (recalling a list of words), logical memory (recalling a phrase in the middle of a paragraph ), associative memory (linking a name to a face ), spatial memory (location of items in a room ), and semantic memory (how many animals you can name in a minute, for example ). My patients almost always come back complaining about the difficulty of the tests. I just smile and nod. The intricacies and nuances of the tests give us important clues about what might be happening inside the brains of patients who are still very early in the process of cognitive change that goes along with age. Most importantly, they enable us to distinguish between normal brain aging and changes that may lead to dementia. One important section of the cognitive testing evaluates the patient‘s sense of smell. Can they correctly identify scents such as coffee, for example? Olfactory neurons are among the first to be affected by Alzheimer's disease.
Specialists also become attuned to other, less quantifiable changes in people on the road to Alzheimer‘s disease, including changes in gait, facial expressions during conversations, even visual tracking. These changes could be subtle and not recognizable to the average person, but someone more skilled can spot them. The trickiest part of the testing is interpreting the results to distinguish among different types of neurodegenerative disease and dementia. Kellyann dissects the test results to try and trace the likely location of the pathology in the brain and the specific neurotransmitters that are involved. Frontal and vascular demen-tias primarily affect the frontal lobe, a region of the brain responsible for executive functioning such as attention, organization, processing speed, and problem solving. So these forms of dementia rob an individual of such higher-order cognitive features.Alzheimer's disease, on the other hand, predominantly affects the temporal lobes, so the most distinct symptoms relate to memory, language, and auditory processing (forming and comprehending speech )although researchers are beginning to identify different possible subtypes of Alzheimer‘s disease, based on which brain regions are most affected. P's disease is a bit different in that it manifests primarily in a movement disorder-deficiency in producing dopamine.

When we have a thought or perception, it's not just one neural network that is responsible for that insight, or that decision, but many individual networks working simultaneously on the same problem. These parallel networks can reach different conclusions, so when we use the expression “ I am of two minds about something " that is not scientifically inaccurate. The brain then picks the most common response. There is redundancy built into the system. The more of these networks and subnetworks that we have built up over our lifetime, via education or experience, or by developing complex skills such as speaking a foreign language or playing a musical instrument, the more resistant to cognitive decline we will tend to be. The brain can continue functioning more or less normally, even as some of these networks begin to fail. This is called “cognitive reserve,” and it has been shown to help some patients to resist the symptoms of Alzheimer's disease. It seems to take a longer time for the disease to affect their ability to function.
There is a parallel concept known as “movement reserve "that becomes relevant with Parkinson's disease. People with better movement patterns, and a longer history of moving their bodies, such as trained or frequent athletes, tend to resist or slow the progression of the disease as compared to sedentary people. This is also why movement and exercise, not merely aerobic exercise, but also more complex activities like boxing workouts are a primary treatment and prevention strategy for P's disease. Exercise is the only treatment that is shown to delay the progression of P's D. But, it can be difficult to disentangle cognitive reserve from other factors, such as socioeconomic status and education, which are in turn linked to better metabolic health and other factors ( also known as" healthy user bias " ). Thus, the evidence on whether cognitive reserve can be trained, or used as a preventive strategy, such as by learning to play a mus instrument or other forms of brain training is highly conflicted and not conclusive-although neither of these hurt, so why not? The evidence suggests that tasks or activities that present more varied challenges, requiring more nimble thinking and processing, are more productive at building and maintaining cognitive reserve. Simply doing a crossword puzzle every day, on the other h, seems to only make people better at doing xword puzzles. The same goes for movement reserve-dancing seems to be more effective than walking at delaying symptoms of P's D, possibly because it involves more complex movement.

There is a growing body of research linking oral health, particularly the state of one's gum tissue, with overall health. Researchers have found that one pathogen in particular, a microbe called P. gingivalis that commonly causes gum disease, is responsible for large increases in levels of inflammatory markers such as lL-6. Even stranger, P. gingivalis has also shown up inside the brains of patients with Alzheimer's D, though scientists are not sure that this bacterium is directly causing dementia. The association is too strong to be ignored. (Also, better oral health correlates strongly with better overall health, particularly in terms of cardiovascular disease risk, so I pay much more attention to flossing and gum health than I used to.
Don't forget saunas. They do help! The more time I spend buried in this literature, the more I become convinced by the magnitude of the benefit, the uniformity of the studies and the mechanisms providing plausibility. Four sessions per week, 20 minutes per session, 82°C or hotter.
Reduce homocysteine with B-vitamins and improve Vitamin-D levels.
At a deeper, more biochemical level, exercise really does act like a drug. To be more precise, it prompts the body to produce its own endogenous drug-like chemicals. When we are exercising, our muscles generate molecules known as cytokines that send signals to other parts of our bodies, helping to trengthen our immune system and stimulate the growth of new muscle and stronger bones. Endurance exercise such as running or cycling helps generate another potent molecule called brain-derived neurotrophic factor, or BDNF, that improves the health and function of the hippocampus, a part of the brain that plays an essential role in memory. Exercise helps with brain vasculature and volume.
Even if exercise doesn't increase your lifespan, it'll increase your healthspan-so you'll have higher QoL.
By age eighty, the average person will have lost eight kilograms of muscle, or about eighteen pounds, from their peak. But people who maintain higher activity levels lose much less muscle-more like 3-4 kg on average. Causation likely goes both ways-there's no chicken and egg.

I find the centenarian decathlon useful because it helps us visualize, with maximum precision, exactly what kind of fitness we need to build and maintain as we get older. It creates a tem- plate for our training. I start by presenting my patients with a long list of physical tasks that might include some of the following:
Dr. Peter Attia’s Centenarian Decathlon:
- Hike 1.5 miles on a hilly trail
- Get up off the floor using a maximum of one arm for support
- Pick up a 30-pound child from the floor
- Carry two five-pound bags of groceries for five block.
- Lift a 20-pound suitcase into the overhead compartment of a plane
- Balance on one leg for 30 seconds with eyes open. (Bonus: eyes closed for 15 seconds)
- Have sex
- Climb four flights of stairs in three minutes
- Open a jar
- Do thirty consecutive jump-rope skips
- Swim half a mile in twenty minutes.
- Walk with a thirty-pound dumbbell in each hand for one minute.
- Draw back and fire a fifty-pound compound bow.
- Do five pull-ups.
- Climb ninety steps in two minutes (VO2 max = 32).
- Dead-hang for one minute.
- Drive a race car within 5 to 8 percent of the pace I can do so today.
- Hike with a twenty-pound backpack for an hour.
- Carry my own luggage.
- Walk up a steep hill.
Their new fat cells sucked up their excess blood glucose and stored it safely.
Think of fat as acting like a kind of metabolic buffer zone, absorbing excess energy and storing it safely until it is needed.
Professional cyclists can use fat almost exclusively for energy even at peak power output. However, diabetics are incapable of burning fat even at moderate intensity. We want to achieve metabolic flexibility through zone 2 training. Fatty acids can be converted to energy only in the mitochondria unlike glucose, which has multiple pathways.
According to Peter Attia, Zone 2 training is a low-intensity, long-duration exercise that is primarily focused on improving the body's ability to burn fat and enhance mitochondrial health. It involves maintaining a heart rate within a specific range, usually 60-70% of maximum heart rate, while exercising at a pace where you can comfortably maintain a conversation.

You need about 3 hrs per week of zone 2 exercise to derive a benefit. I am so persuaded by the the benefits of zone 2 that it has become a cornerstone of my training plan. Four times a week, I will spend about an hour riding my stationary bike at my zone 2 threshold. One way to track your progression in zone 2 is to measure your output in Watts at this level of intensity. Many stationary bikes can measure your wattage as you ride. You take your average wattage output for a zone 2 session and divide it by your weight to get your watts per kilogram, which is the number we care about. So, if you weigh 60 kilos (about 132 lbs) and can generate 125 watts in zone 2, that works out to a little more than 2W/kg, which is what one would expect from a reasonably fit person. These are rough benchmarks. Someone who is very fit will be able to produce 3W/kg while a pro cyclist can do 4W/kg. It's not the number but how much you're improving.

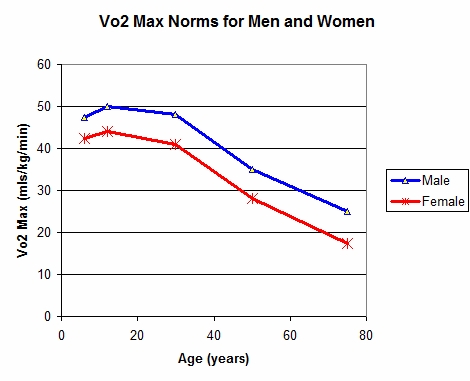
Our VO2 max is a pretty good proxy for a measure of our physical capability.. it tells us what we can do and what we cannot do. First, there's a huge gap in fitness between top and bottom 5% of each group. It's striking how steeply VO2 max declines with age, and how this decline corresponds with diminished functional capacity. Lower it goes, less you can do. E.g. A 35 year old man with average fitness for his age-VO2 max in mid 30's should be able to run at 6 mph. But, at age 70, only the very fittest 5% of people will still be able to manage this. Likewise, average 45-50 year old will be able to climb stairs slowly-VO2 max of 32, but at 75, such a feat demands that a person be in the top tier of their age group. Activities that are easy when we are young or middle aged become difficult if not impossible as we get older.
Anyone can improve VO2 max, and they should, because the alternative is so unacceptable. Once maximal oxygen consumption or VO2 max drops below a certain level (typically about 18 ml/kg/min in men, and 15 in women ), it begins to threaten your ability to live on your own. Your engine is beginning to fail. This is why it's important to train VO2 max in addition to zone 2.
How trainable is VO2 max? The conventional wisdom, reflecting the bulk of the literature, suggests that it's possible to improve elderly subjects' aerobic capacity by about 13 percent over eight to ten weeks of training, and by 17% after 24-52 weeks. That's a good start but represents only the beginning of what is possible. We are talking about a lifelong training program.
Peter Attia recommends a balanced approach to training VO2 max, combining Zone 2 training and High-Intensity Interval Training (HIIT). He suggests dedicating 80% of training time to Zone 2 and 20% to HIIT. This approach focuses on building a strong aerobic base (Zone 2) while also improving VO2 max through high-intensity efforts.
The tried and true formula for these intervals is to go 4 minutes at the max you can sustain for this amount of time, not an all out sprint, but still a very hard effort, then ride or jog for 4 min easy, which should be enough time for your heart rate to come back down to below about 100 bpm. Repeat this for 4-6 times and then cool down.
In practice, I found that my ideal VO2 max pace works out to about 33% more power than my zone 2 pace-if I'm doing 4 on, 4 off intervals. So, if your zone 2 pace is 150 Watts, your VO2 max pace should be about 200 W.
Rucking is a practical way to add carrying back into our lives. " The main difference is that instead of carrying sixty pounds of antelope meat in my pack, l'm typically hauling heavy metal weights, which are admittedly less appetizing. One thing I specifically focus on when rucking is the hills. Going uphill gives me a chance to push my VO2 max energy system; first-time ruckers are amazed at how taxing it is
I find that spending time moving in nature, simply enjoying the feeling of the wind in my face and the smell of the budding spring leaves (and a heavily loaded pack on my back) helps me cultivate what Ryan Holiday calls “stillness,” the ability to remain calm and focused amid all the distractions that our world offers and that we create for ourselves. When my family comes along, it's important bonding time
I am semi obsessed with rucking-hiking at a fast pace with a loaded pack on your back. 3-4 days a week, I'll spend an hour rucking around my neighborhood, up and down hills, typically climbing and descending several hundred feet over 3-4 miles. The 50-60 lbs pack on my back makes it quite challenging, so I'm strengthening my legs and my trunk, while also getting in a solid cardio session. Best part is that I never take my phone on these outings. It's just me, in nature, or maybe with a friend or family member or houseguest, for whom rucking is mandator-I keep two extra rucksacks in the garage. I was introduced to this by Michael Easter in his eye-opening "The Comfort Crisis".
Beth Lewis - the Art of Toe Yoga

Trainers can be helpful in teaching you the basics of exercises and to motivate you to get into the habit of working out, but if you never learn to do the exercises on your own or never try different ways of doing them, you will never develop the proprioception needed to master your ideal movement patterns. You will rob yourself of the learning progression that is such an important part of stability training-process of narrowing the gap between what you think you are doing and what you are actually doing. I swear by my smartphone and tripod. I film the ten most important sets of the day and review the recording between sets to see the gap between what I did and what I think I did.
Diet and nutrition are so poorly understood by science, so emotionally loaded, and so muddled by lousy information and lazy thinking that it is impossible to speak about them in nuanced terms at a party, or, say, on social media. Yet, most people these days are conditioned to want bullet point listicles, bumper sticker slogans or other superficial forms of analysis. It reminds me of a story the great physicist and one of my heroes-Richard Feynman. Being asked at a party to explain, briefly and simply, why he was awarded the Nobel Prize. He responded that, if he could explain his work briefly and simply, it probably wouldn't have merited a Nobel Prize. Feynman's rule also applies to nutrition. We actually know far less about this subject than we do about subatomic particles.
While fat restriction also limits food choices, it can be less effective at reducing appetite if you pick the wrong low-fat foods to eat ( e.g., high-carb junk food ). If you consume most of your carbohydrates in the form of fruit loops, for example, you will still be very hungry all the time. A major risk with DR is that you can still easily end up overnourished if you are not deliberate about it. People tend to ( erroneously ) assume you can't eat too much if you're jsut restricting ____ (for e.g. carbohydrate). This is incorrect. Even if done correctly and strictly, DR can still result in overnutrition. If you cutout carbohydrates altogether but overdo it on the Wagyu steaks and bacon, you will fairly easily find yourself in a state of caloric excess. The key is to pick a strategy to which you can adhere, but which also helps you reach your goals. This takes patience, some willpower and a willingness to experiment. We also want to be sure we're not compromising our other goals along the way. Any form of DR that restricts protein, for example, is probably a bad idea for most people, because it likely also impairs the maintenance or growth of muscle. Similarly, replacing carbs with lots saturated fats can backfire if it sends your APO(b) concentration and thus your CVD risk sky high. A more significant issue with DR is that everyone's metabolism is different. Results vary. Exact same diet can see some people benefit, but others see their lipid markers go up. Conversely, some people might lose weight on a low-fat diet, while others will gain weight. l have seen this happen time and again in my own practice, where similar diets yield very different outcomes, depending on the individual. For example, when Eduardo, the 40-year-old construction worker with a soccer player build who consumed six bottles of gatorade a day, came to see me, with what turned out to be a full-blown case of type-2 diabetes, type 2 diabetes, cutting his carbohydrate intake was clearly the way to go. Type-2 D is a condition of impaired carb metabolism after all. From the outside, he seemed pretty healthy. He didn't fit the stereotype of the lazy gluttonous diabetic, but he had no ability to store the excess sugar that he consumed. His H-A1C was 9.7%, well into the diabetic red-zone. Being latino, he was at higher risk of NAFLD to begin with.
Insights Dr. A gained from Continuous Glucose Monitoring
 |
- Not all carbs are created equal - more fibre - lower glycemic index - I do at least 50 grams of fibre a day
- Rice and oatmeal is bad and brown rice only slightly better
- Fructose doesn't show up in CGM
- Timing, duration, and intensity of exercise matter a lot. In general, aerobic exercise seems most efficacious at removing glucose from circulation, while high-intensity exercise and strength training increase glucose transiently because liver sends glucose into blood-don't be alarmed
- Sleep matters a lot - just 5-6 hrs vs 7-8 hrs counts for a 10-20 mg/dl jump in peak glucose response and a 5-10 mg/dl response in overall levels
- Stress (maybe due to cortisol) has a big influence on blood glucose
- Non starchy veggies like spinach and broccoli have no impact on blood sugar
- Foods high in protein and fat have no effect in blood sugar, but large amounts of lean protein will elevate blood glucose slightly. Protein shakes esp if low in fat, will have a big effect.
- Stacking above insights in both directions (+ve or -ve) is powerful - so if you're stressed out, sleeping poorly and unable to make time to exercise, be very careful with what you eat
- Most important - simply tracking glucose has positive impact on behavior - Hawthorne effect
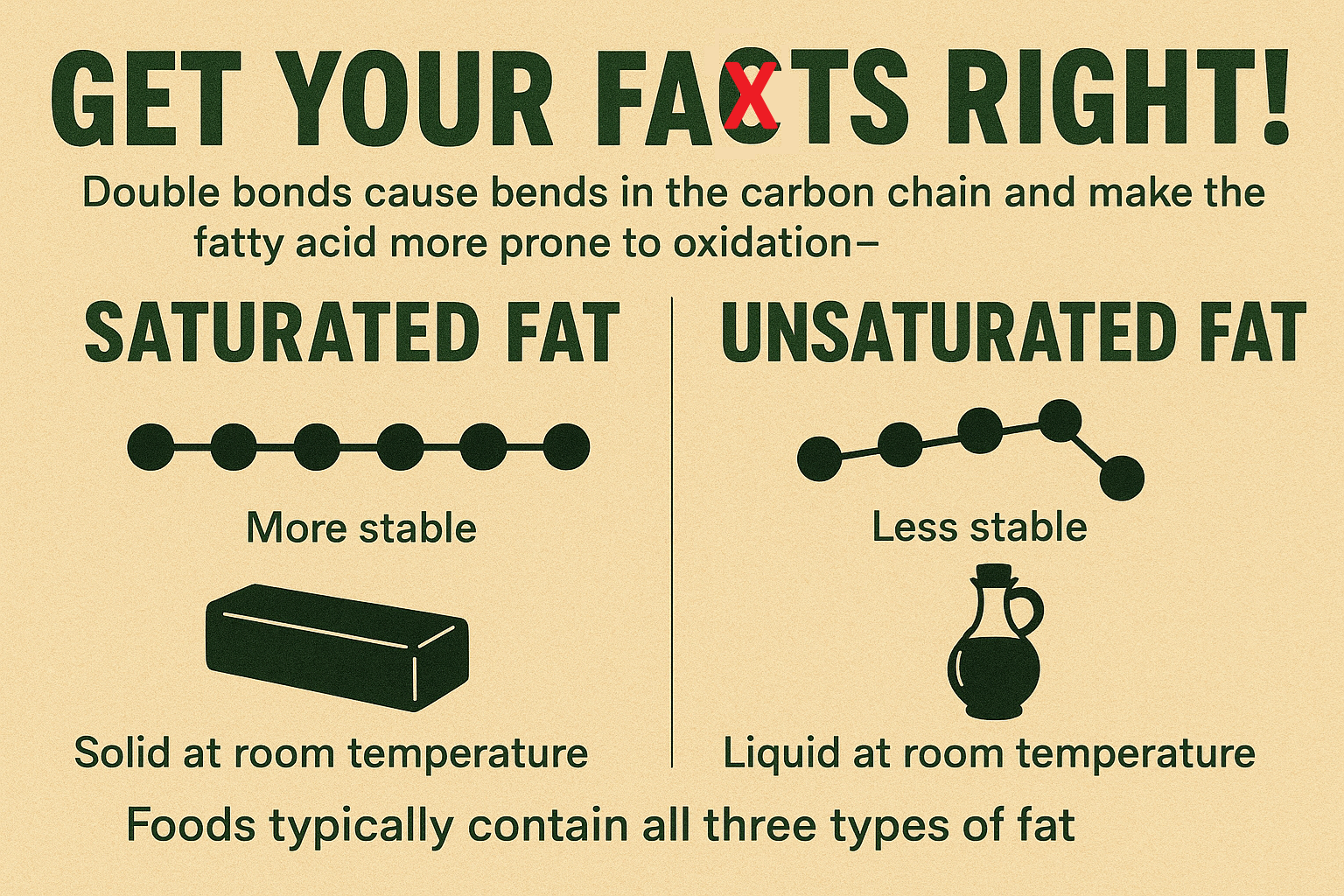
Double bonds cause bends in the carbon chain and make the fatty acid more prone to oxidation. Saturated fats are more stable and do not easily react with other molecules. Since saturated fats are linear and can be densely packed together, they can be more solid at room temperature. Because unsaturated fats have kinks in their structure, they are more likely to be liquid at room temperature. Key to remember, and somehow, almost always overlooked, is that no food belongs to just one group of fats. Olive and safflower oils might be as close as you can get to a monounsaturated fat, while palm and coconut oil might be as close as you can get to a pure saturated fat. But, all foods containing fats typically contain all three types of fat.

Setting time limits around food consumption helps foil a key feature of the SAD (Seasonal Affective Disorder), which is that it's difficult to stop eating it. Time-restricted feeding is a way of putting the brakes on snacking and late-night meals-type of mindless eating just to eat-that the Japanese call "kuchisabishii"-lonely mouth.
Scary as it can be in some situations, the short-term harm done by a night or three of poor sleep pales in comparison to the damage that we do to ourselves if this situation continues. Kirk Parsley observed this when he was a physician to the SEALS. Outwardly, these men appeared to be prime physical specimens, finely honed by their rigorous training. But when Parsley analyzed their blood tests, he was shocked; many of these young guys had the hormone levels and inflammatory markers of men several decades older than them “old-man blood," Parsley called it. Because their training exercises and missions often began at odd hours of the night and required them to stay awake for twenty-four hours or more at a stretch, they were chronically sleep deprived. their natural sleep-wake cycles utterly disrupted.
When Kirk told me that story, I experienced a jolt of recognition: I, too, had had “old-man blood,” during my Not-Thin Peter phase. with elevated insulin, high triglycerides, and a testosterone level in the bottom 5 percent of men in the United States. I had always attributed my poor health and hormone imbalance at that point to my lousy diet. and diet alone, but I had also spent at least a decade in a state of severe sleep deprivation, in residency and afterward.
https://thealaskabear.com
Another way to turn down the sympathetic nervous system and prepare the brain for sleep is through meditation. There are several very good apps that can help with guided meditations, including some that are focused entirely on sleep. Personally, I have found sauna use in the evening to be one of the most potent tools to help prepare me for sleep-both because of the temperature effects which we discussed earlier and because it is a forced reckoning away from work. Overarching point-good night of sleep may depend on a good day of wakefulness-one that includes exercise, outdoor time, sensible eating, minimal to no alcohol, stress management, knowing where to set boundaries around work and other life stressors.
Sleep rules :
- No alcohol - if you must, one drink before 6 PM. It impairs sleep quality much more than anything. Don't confuse the drowsiness it produces with quality sleep
- No food within 3 hours of bedtime, preferably longer. Best to go to bed with a bit of hunger, too much can distract.
- No screen time beginning two hours before bed. Also, block blue light after dark.
- For at least one hour before bed, avoid stimulating or anxiety producing work (social media)
- Sauna or hot-tub. Hot bath or shower also works
- Room should be cool - ideal mid 60's. Bed should also be cool - use cool mattress or one of the bed cooling devices out there.
- Darken room completely - shouldn't be able to see your hand before your face. If that is not achievable, use silky (Alaska Bear) eyeshade
- Give yourself enough sleep opportunity time - means go to bed at least 8 hours before you need to wake
- Fix wake up time and don't deviate from it even on weekends
- Don't obsess over sleep.
Trauma falls into five categories
- abuse (physical or sexual, but also emotional or spiritual)
- neglect
- abandonment
- enmeshment (the blurring of boundaries between adults and children )
- witnessing tragic events
Bit T and little T. Having an alcoholic parent subjects the child to lots of little-T traumas. In large enough doses, little-T traumas can shape a person's life just as much as one major terrible event.

David Brooks' "The Road to Character": On the plane, I read the part where Brooks makes a key distinction between "resume virtues," meaning the accomplishments that we list on our CV, our degrees and fellowships and jobs, versus “eulogy virtues,“ the things that our friends and family will say about us when we are gone.
The over-arching theme is mindfulness, which gives you the ability to work through the other four: emotional regulation (getting control over our emotions), distress tolerance (our ability to handle emotional stressors)
workbook with a DBT therapist, doing exercises every day. I'm better at doing than thinking sometimes. The practice of DBT is predicated on learning to execute concrete skills, repetitively, under stress, that aim to break the chain reaction of negative stimulus -> negative emotion -> negative thought -> negative action. DBT consists of four pillars joined by one overarching theme. The over-arching theme is mindfulness, which gives you the ability to work through the other four:
- emotional regulation (getting control over our emotions)
- distress tolerance (our ability to handle emotional stressors)
- Interpersonal effectiveness (how well we make our needs and feelings known to others)
- Self-management (taking care of ourselves - beginning with basic tasks like getting up in time for going to school)
No comments:
Post a Comment